GLP-1 Drugs and Bodybuilding: How to Preserve Muscle on Semaglutide and Tirzepatide
GLP-1 bodybuilding isn’t just a trend — it’s a legitimate cutting strategy with one serious catch. Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) produce rapid fat loss, but clinical trials consistently show 26–40% of total weight loss comes from lean mass, not fat. For someone who’s spent years building muscle, that’s an unacceptable ratio. This guide gives you the bodybuilder-specific protocol for running a GLP-1 agonist for a hard cut without gutting your muscle mass in the process.
WHAT YOU’LL LEARN IN THIS GUIDE
– Why GLP-1 drugs cause muscle loss and how significant the risk actually is
– The protein intake threshold needed to preserve lean mass on semaglutide or tirzepatide
– How to structure training on a GLP-1 cut to retain strength and muscle
– 2026 research on bimagrumab + semaglutide combinations for near-zero muscle loss
– Whether stacking BPC-157 or other peptides with GLP-1s is worth it
– SARMs + GLP-1 combinations — what bodybuilders are actually running
– The weekly check-in protocol to monitor muscle vs fat loss ratio
The Short Answer
THE SHORT ANSWER
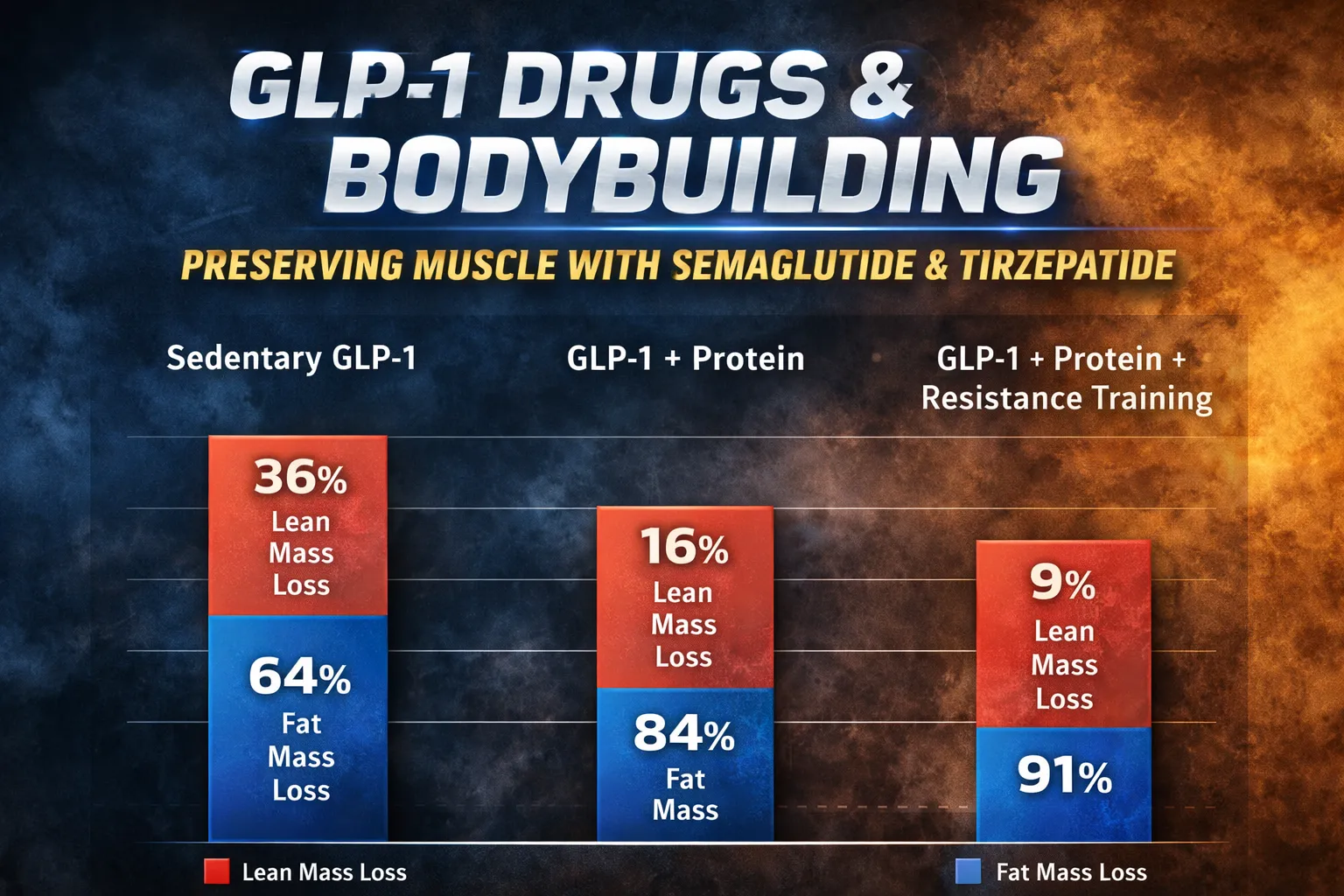
GLP-1 bodybuilding is viable for cutting phases when protein intake is kept at 1.2–1.6g per pound of bodyweight daily and resistance training is maintained at 3–4 sessions per week. Without these two interventions, semaglutide and tirzepatide can cause significant lean mass loss — clinical data shows 26–40% of total weight loss comes from muscle in sedentary users. With consistent heavy training and high protein, that ratio improves dramatically and most of the weight loss comes from fat.
[IMAGE SUGGESTION 1: A body composition comparison chart showing three groups — sedentary GLP-1 users, GLP-1 + protein, and GLP-1 + protein + resistance training — comparing fat loss vs lean mass loss percentages over 12 weeks, with clear color differentiation.]
1. How GLP-1 Drugs Work and Why They Affect Muscle Mass
GLP-1 agonists work by mimicking glucagon-like peptide 1, a hormone naturally released in the gut after eating. They slow gastric emptying, suppress appetite, improve insulin sensitivity, and reduce caloric intake — often dramatically. The average user on semaglutide loses 15–20% of total body weight. On tirzepatide (a dual GLP-1/GIP receptor agonist), weight loss reaches 20–22% in clinical trials.
The muscle loss issue stems from the mechanism itself. GLP-1 agonists don’t preferentially burn fat — they create a calorie deficit, and the body loses weight from whatever stores are most accessible. Without the anabolic signals of resistance training and adequate protein, a significant portion of that weight loss comes from skeletal muscle tissue.
| GLP-1 Drug | Mechanism | Average Total Weight Loss | Lean Mass Loss (Sedentary) | Lean Mass Loss (Training + High Protein) |
|---|---|---|---|---|
| Semaglutide (Ozempic/Wegovy) | GLP-1 receptor agonist | 15–17% | 30–40% of total loss | 10–15% of total loss |
| Tirzepatide (Mounjaro/Zepbound) | GLP-1 + GIP dual agonist | 20–22% | 26–36% of total loss | 8–12% of total loss |
| Retatrutide (Eli Lilly, Phase 3) | GLP-1 + GIP + Glucagon triple | 24–26% (early data) | Data pending | Data pending |
| Pemvidutide (Phase 3, 2026) | GLP-1 + Glucagon dual | 15–17% | Less than 10% of total loss (by design) | Est. 5–8% |
WHAT THE RESEARCH SAYS
A 2026 Cell Reports Medicine study on both mice and humans found that GLP-1 medicines do not cause disproportionate loss of muscle mass relative to overall weight loss in obese subjects. However, the key phrase is “relative to overall weight loss” — not “relative to a goal of zero muscle loss.” For bodybuilders who want to preserve maximum lean tissue, the absolute muscle loss still needs to be addressed through dietary and training interventions.
2. The Protein Threshold for Muscle Preservation on GLP-1 Agonists
GLP-1 bodybuilding protocol starts with one non-negotiable: protein intake. This is where most GLP-1 users fail. The drug crushes appetite so effectively that people undereat everything, including protein. When you’re running semaglutide or tirzepatide at therapeutic doses, you may naturally only want to eat 1,200–1,600 calories a day. If those calories aren’t prioritized toward protein, muscle loss is unavoidable.
| Body Weight | Minimum Protein Target (1.2g/lb) | Optimal Protein Target (1.6g/lb) | Recommended Meal Distribution |
|---|---|---|---|
| 170 lbs | 204g/day | 272g/day | 4 meals × 50–68g |
| 190 lbs | 228g/day | 304g/day | 4–5 meals × 57–76g |
| 210 lbs | 252g/day | 336g/day | 5 meals × 50–67g |
| 230 lbs | 276g/day | 368g/day | 5–6 meals × 55–73g |
Research from Mass General Hospital supports aiming for at least 30g of protein per meal to clear the minimum threshold for muscle protein synthesis activation. On GLP-1 agonists where appetite suppression is severe, prioritizing protein in the first portion of every meal — before carbs or fats — is a practical strategy to ensure the target is hit even when total food intake is low.
GYM APPLICATION
On days when semaglutide or tirzepatide kills your appetite entirely, use a high-protein meal replacement or protein shake with 50g+ of protein as your first “meal” of the day. This guarantees the anabolic signaling threshold is hit even before hunger returns. Casein-based shakes work particularly well because slower digestion keeps amino acid levels elevated longer — useful when meal frequency is low due to appetite suppression.
3. How to Structure Training for GLP-1 Bodybuilding
The STEP-UP substudy data on semaglutide is unambiguous on this point: participants who combined resistance training with GLP-1 therapy retained 85% of their lean mass over a 12-week program. Sedentary participants retained only 55%. For a bodybuilder, this translates directly into a training requirement during any GLP-1 cut.
Training Frequency and Volume on GLP-1 Agonists
Because you’re in a significant calorie deficit on GLP-1s, your recovery capacity is reduced compared to a maintenance or bulk phase. The training goal shifts from growth-maximizing to muscle-preserving — which means keeping volume sufficient to provide the anabolic stimulus without exceeding what you can recover from on a restricted diet.
- Frequency: 3–4 resistance training sessions per week minimum. More than 5 sessions becomes counterproductive when calories are this low.
- Sets per muscle per week: 12–16 sets (natural minimum effective volume). Don’t try to run the same high volume you’d use on a bulk — you won’t recover.
- Intensity: Maintain or slightly increase load on compound movements. Reducing weight is the fastest path to muscle loss signal — your body needs the heavy mechanical tension to prioritize muscle retention.
- Cardio: Keep cardio to Zone 2 (low intensity, 2–3 sessions, 30 min max). High-intensity cardio adds to the calorie deficit and competes with muscle retention when protein is already constrained.
[IMAGE SUGGESTION 2: A weekly training template for GLP-1 cutting phase showing 4 training days, exercise selection, volume targets, cardio days, and rest days in a visual weekly calendar format.]
Exercise Selection Priority on GLP-1 Cuts
When calories are low and recovery is limited, exercise selection becomes more important. Prioritize compound movements that train multiple muscle groups simultaneously — these give you the most muscle retention signal per unit of recovery cost.
| Priority | Movement | Why It Matters on GLP-1 Cut |
|---|---|---|
| 1 | Squat (back or front) | Highest lower body muscle retention signal; massive testosterone and GH response |
| 2 | Deadlift or Romanian Deadlift | Full posterior chain activation; preserves glutes, hamstrings, back simultaneously |
| 3 | Bench Press or Weighted Dips | Chest + tricep + anterior delt preservation in one movement |
| 4 | Barbell or DB Row | Upper back preservation; prevents the “skinny fat” look during calorie restriction |
| 5 | Overhead Press | Shoulder and trap preservation; keeps upper body structure during weight loss |
| 6 | Pull-Up or Lat Pulldown | Lat and bicep retention with minimal recovery cost |
4. The 2026 Research: Bimagrumab + Semaglutide for Near-Zero Muscle Loss
One of the most significant developments in GLP-1 bodybuilding science is the combination of semaglutide with bimagrumab — an anti-activin type II receptor antibody that inhibits myostatin and ActRII signaling. In clinical trials, this combination produced weight loss almost entirely from adipose tissue, with less than 10% of lost weight coming from lean mass. Participants actually gained muscle in some subgroups while losing significant fat.
WHAT THE RESEARCH SAYS
A 2025 American Diabetes Association presentation reported that bimagrumab + semaglutide combination produced over 90% of weight loss as pure fat in Phase 2 trial subjects, compared to approximately 60–70% fat loss in semaglutide-only groups. This is the closest pharmacological approach yet to the “body recomposition while cutting” effect that bodybuilders have long sought from compound stacking.
Bimagrumab is not yet commercially available as of April 2026, but the Phase 3 trial data expected later in 2026 may accelerate approval. For bodybuilders, this is the next compound to watch closely. Pemvidutide, which targets GLP-1 and glucagon receptors simultaneously, is also showing dramatically reduced lean mass loss compared to standard GLP-1 monotherapy and received FDA Breakthrough Therapy designation for MASH in January 2026.
5. BPC-157 and Peptide Stacking With GLP-1 Agonists
GLP-1 agonists cause significant GI side effects — nausea, delayed gastric emptying, and gut motility changes that can make eating enough protein genuinely difficult. Some bodybuilders are stacking BPC-157 (Body Protection Compound 157) with their GLP-1 protocol to mitigate GI side effects and improve gut function.
BPC-157 is a pentadecapeptide derived from human gastric juice that has been studied for its effects on gut healing, GI motility, and inflammation. It acts on the vagus nerve and has been shown in animal models to improve gastric emptying and reduce gastric ulcer formation. For bodybuilders on GLP-1 agonists experiencing severe nausea or gastroparesis-like symptoms, BPC-157 may provide partial relief and improve the ability to hit protein targets.
⚠️ SAFETY NOTE
There are no published clinical trials on BPC-157 and GLP-1 agonist co-administration in humans. The combination is based on anecdotal bodybuilding community reports and mechanistic reasoning, not controlled data. If you experience severe GI symptoms on semaglutide or tirzepatide, discuss dose reduction with your prescribing physician before adding additional compounds.
6. SARMs + GLP-1 Combinations: What Bodybuilders Are Actually Running
The bodybuilding community has developed a pragmatic approach to GLP-1 muscle preservation that involves combining GLP-1 agonists with anabolic compounds specifically chosen for their muscle-sparing properties. The most commonly reported stacks are:
| Compound | Role in GLP-1 Stack | Why It’s Used | Reported Dosage |
|---|---|---|---|
| Ostarine (MK-2866) | Muscle preservation SARM | Mild anabolic effect protects lean mass during calorie deficit; minimal suppression at low dose | 12.5–25mg/day |
| MK-677 (Ibutamoren) | GH pulse stimulator | GH elevation during GLP-1 cut helps preserve lean mass and improve fat oxidation simultaneously | 10–25mg/night |
| Cardarine (GW-501516) | Fat oxidation enhancer | PPAR-delta agonist improves fatty acid oxidation without muscle catabolism; enhances GLP-1 fat loss | 10–20mg/day |
| Low-dose Testosterone | Anabolic anchor | TRT-level testosterone (125–200mg/week) preserves lean mass, libido, and energy during aggressive cut | 125–200mg/week |
The most evidence-supported of these is the combination of a GLP-1 agonist with low-dose testosterone or an anabolic-preserving SARM like Ostarine. The logic is sound: GLP-1 handles the calorie deficit mechanism, while the anabolic compound handles the lean mass preservation signal. Resistance training provides the mechanical stimulus that tells the body which tissue to protect.
7. The Weekly Check-In Protocol for Monitoring Muscle vs Fat Loss
Running a GLP-1 bodybuilding protocol without tracking body composition is flying blind. You need to know whether the weight coming off is fat or muscle on a weekly basis, not just at the end of a 12-week cut.
Weekly Monitoring Metrics
- Body weight (same conditions, daily morning average) — Track 7-day rolling average to eliminate water weight noise
- Training performance log — If strength on key compound lifts (squat, bench, deadlift) drops more than 5–8% from week to week, you’re losing muscle-driving neural capacity
- Visual body composition check — Monthly side-view and front photos in consistent lighting; muscle separation should be maintained or improving as fat drops
- DEXA scan every 6–8 weeks — The gold standard for tracking lean mass vs fat mass. DEXA is affordable ($40–80 at most sports medicine clinics) and gives you actual data
- Bloodwork at 8 weeks minimum — Check testosterone, LH, IGF-1, albumin, and key metabolic markers. Aggressive cutting on GLP-1s with inadequate protein can tank testosterone and IGF-1 levels
GYM APPLICATION
If your squat or deadlift drops more than 10% from your starting weight during a GLP-1 cut without any change in training, that’s a strong signal of lean mass loss rather than just fatigue. Respond immediately: increase protein by 20g/day and reduce the GLP-1 dose by half for 2 weeks, then reassess. Chasing weight loss numbers at the expense of strength is the fastest way to look “skinny fat” instead of lean and muscular when you’re done cutting.
8. GLP-1 Dosing Strategy for Bodybuilders
Most GLP-1 prescriptions follow a clinical titration schedule designed for obese patients, not bodybuilders cutting from 15% to 8% body fat. Bodybuilders often need a different approach to dosing to maintain the calorie deficit without the side effects that tank protein intake.
| Semaglutide Dose | Calorie Suppression Effect | GI Side Effects | Bodybuilder Use Case |
|---|---|---|---|
| 0.25mg/week | Mild (200–400 kcal/day) | Minimal | Ideal starting dose for lean individuals; enough deficit without crushing appetite |
| 0.5mg/week | Moderate (400–600 kcal/day) | Mild to moderate | Most effective range for bodybuilders; manageable side effects |
| 1.0mg/week | Strong (600–900 kcal/day) | Moderate to significant | Use only if body fat is significantly elevated; protein targeting becomes harder |
| 2.0–2.4mg/week | Very strong (800–1200+ kcal/day) | Often severe | Generally not appropriate for lean bodybuilders; lean mass risk is high |
For bodybuilders already at relatively low body fat (10–15%), the 0.25–0.5mg/week range is typically more appropriate than the maximum clinical doses. The goal is a controlled, sustainable deficit that allows protein targets to be met — not maximum weight loss speed.
Common Mistakes When Running GLP-1 Bodybuilding Protocols
| Mistake | Why It Destroys Muscle | What to Do Instead |
|---|---|---|
| Letting appetite suppression prevent protein eating | Without adequate amino acid availability, muscle protein breakdown exceeds synthesis regardless of training | Prioritize protein in every meal before carbs/fats; use liquid protein if solid food is hard |
| Using GLP-1 maximum clinical doses when already lean | At 0–15% body fat, the body has limited fat stores to tap; muscle becomes the path of least resistance | Use minimum effective dose (0.25–0.5mg semaglutide) and increase only if fat loss stalls |
| Replacing resistance training with cardio on a GLP-1 cut | Cardio signals aerobic adaptation, not muscle preservation; without mechanical tension, muscle loss accelerates | Keep 3–4 resistance sessions per week; cardio is supplemental only |
| Not tracking strength metrics during the cut | Muscle loss happens silently — you won’t feel it until it’s gone if you don’t track performance | Log every training session; treat 10%+ strength decline as a red flag |
| Stopping the GLP-1 abruptly without a plan | Appetite returns rapidly; without protocol, most people regain weight quickly and in fat-dominant form | Taper dose over 4–6 weeks; maintain training and protein protocols through the transition |
Article Summary
- GLP-1 agonists like semaglutide and tirzepatide cause 26–40% of total weight loss from lean mass in sedentary users — this is the core problem for bodybuilders
- Resistance training 3–4x per week combined with high protein (1.2–1.6g/lb) can reduce lean mass loss percentage to 8–15% of total weight lost
- Protein intake must be actively prioritized — appetite suppression from GLP-1 drugs makes it easy to undereat protein catastrophically
- Aim for 30g+ protein per meal minimum; use liquid protein sources when appetite suppression is severe
- Compound movements (squat, deadlift, bench, row) provide the mechanical tension signal that tells the body to preserve muscle during caloric restriction
- Use the lowest effective GLP-1 dose when already lean — maximum clinical doses are not appropriate for bodybuilders at 10–15% body fat
- Bimagrumab + semaglutide combination shows near-zero lean mass loss in Phase 2 data — watch for Phase 3 results in late 2026
- BPC-157 may mitigate GI side effects that prevent adequate protein intake, but clinical data for this combination is absent
- Monitor strength weekly; a 10%+ decline in compound lift performance is a signal of meaningful muscle loss
- DEXA scans every 6–8 weeks provide the only reliable objective measure of lean mass vs fat mass changes on cycle
Frequently Asked Questions
Can bodybuilders use GLP-1 drugs for cutting without losing muscle?
Yes, but it requires a deliberate protocol. GLP-1 bodybuilding for cutting is viable when you maintain resistance training 3–4x per week and hit protein targets of 1.2–1.6g per pound of bodyweight daily. Without these two factors in place, lean mass loss is significant and clinically documented. With both factors, most of the weight loss comes from fat, and lean mass retention is high. The drug creates the deficit; your training and protein intake determines what’s lost.
Is tirzepatide better than semaglutide for muscle preservation?
Tirzepatide (Mounjaro, Zepbound) shows slightly better lean mass retention data than semaglutide in head-to-head clinical comparisons, possibly due to its additional GIP receptor agonism which may have distinct effects on muscle and fat tissue. In the SURMOUNT trials, tirzepatide users in the training + high protein groups showed approximately 8–12% lean mass loss as a percentage of total loss, compared to 30–40% for sedentary users. However, the differences with semaglutide become small when both groups exercise and eat adequate protein.
How much protein do you need on semaglutide to prevent muscle loss?
The research threshold for meaningful muscle protein synthesis is at least 30g per meal, with a daily total of 1.2–1.6g per pound of bodyweight for active individuals in a calorie deficit. For a 190-pound lifter on semaglutide, that means 228–304g of protein per day — a target that becomes challenging when appetite suppression is severe. Liquid protein sources, protein-prioritized meals, and strategic meal timing become essential tools to hit this number when total caloric intake is restricted.
Should I run Ostarine with semaglutide to preserve muscle?
Ostarine (MK-2866) at 12.5–25mg/day is the most commonly reported SARM addition to GLP-1 bodybuilding protocols for muscle preservation. Its mild anabolic effect on muscle and bone tissue creates an anabolic signal during the calorie deficit without the cardiovascular or liver burden of stronger compounds. That said, there is no clinical trial data on this combination, and the interaction between GLP-1 receptor agonism and androgen receptor modulation has not been formally studied. Use with awareness of the unknown interaction profile.
What happens if you stop semaglutide after a bodybuilding cut?
Appetite returns rapidly after stopping semaglutide, often within 2–4 weeks. Without a structured transition plan, most users regain weight — and the regained weight tends to be disproportionately fat rather than muscle, worsening body composition. For bodybuilders, a 4–6 week dose taper (reducing by 50% every 2 weeks) combined with a gradual calorie increase back to maintenance prevents the rapid rebound. Maintaining protein intake and training frequency through the transition is critical.
Can you use GLP-1 drugs during a SARMs cycle?
Some bodybuilders run GLP-1 agonists during a SARMs cutting cycle, using the SARM for muscle preservation and the GLP-1 for calorie deficit creation. Ostarine and Cardarine are most commonly paired with semaglutide for this purpose. The combination theoretically addresses both sides of the body recomposition equation — anabolic preservation from the SARM plus aggressive fat loss from the GLP-1. There is no clinical data on this combination, and the hormonal interactions between selective androgen receptor modulation and GLP-1 agonism are unstudied. If using this approach, bloodwork monitoring becomes especially important.
Does GLP-1 therapy affect testosterone levels in men?
There is emerging evidence that GLP-1 agonists may modestly improve testosterone levels in obese men by reducing fat mass (adipose tissue is a significant source of aromatase activity that converts testosterone to estrogen). However, aggressive calorie restriction combined with GLP-1 therapy can lower IGF-1 and GH pulse amplitude, which may reduce anabolic signaling. For bodybuilders, this is another reason to prioritize protein and monitor bloodwork during extended GLP-1 cutting phases.
Disclaimer: This article is for informational and educational purposes only. It is not medical advice. The compounds and protocols discussed may carry serious health risks. Always consult a qualified healthcare provider before starting any new supplement, peptide, hormone, or training protocol. GLP-1 medications are prescription drugs and must be obtained through a licensed healthcare provider. FitScience does not encourage or endorse the use of any substances outside of their approved medical indications.

